

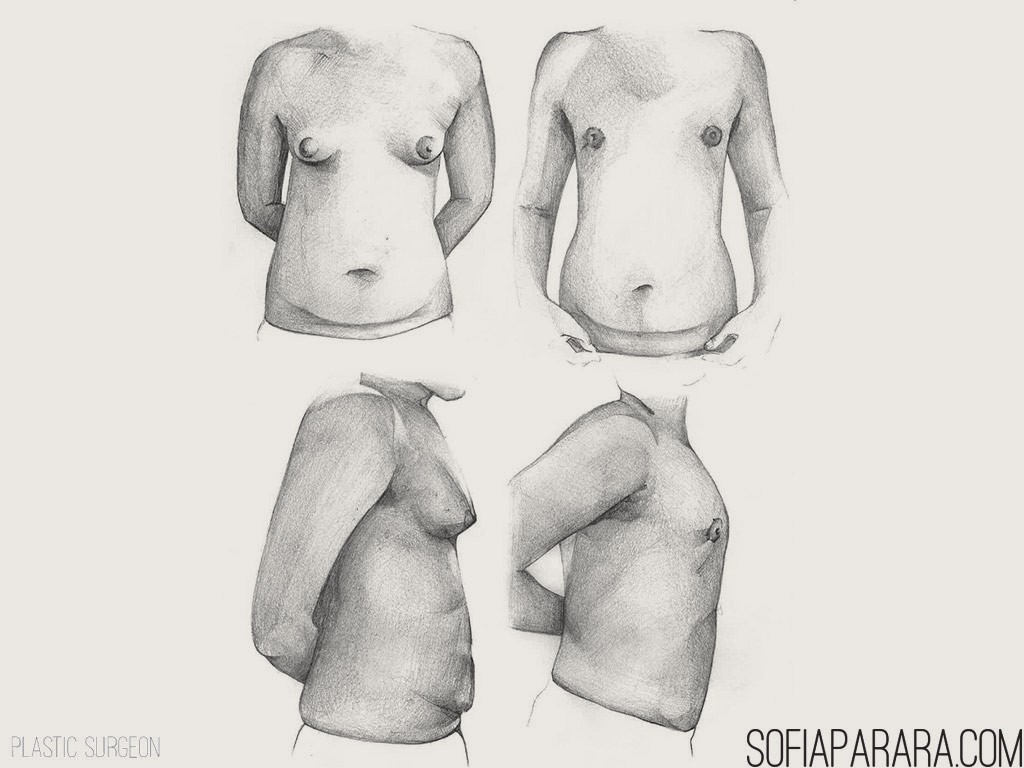
Gynecomastia (woman-like breast) is an extremely common condition occurring in approximately 50% of all men. The degree of the condition may vary from a small nodule of breast tissue behind the nipple-areola complex to real female like breasts of mixed fat and/or glandular tissue.
Certain medical conditions can cause the problem as well as certain medication for example anabolic steroids. The etiology of gynecomastia should be investigated and treated before surgery is considered. Suitable candidates for surgery should ideally have a stable weight and be emotionally balanced.
The operation
Depending on the degree and whether the problem is mainly caused by excess fat and/or gland the problem can either be corrected by liposuction only (mainly fatty tissue) or surgical removal of the glandular tissue or in some cases a combination of the two. The aim is to create a male shaped breast without removing excessive tissue that can cause a contour deformity.
An incision on the edge of the areola is normally used for surgical removal while an incision in the side of the breast or the edge of the areola can be utilized for liposuction. In extreme cases more skin around the areola as well as perpendicularly from the nipple-areola complex, may have to be removed and then scarring in that case will be more extensive.
The procedure is normally performed as a day case procedure under general anaesthetic in the hospital. If large amounts of glandular tissue are removed an overnight stay may be required. Surgical drains are usually inserted overnight in cases of glandular resection.
The wounds are normally covered by a dressing and you may be required to wear a compression garment for up to 6 weeks post surgery. Pain is normally mild and can easily be controlled by adequate medication.
Complications
• Infection occurs rarely but you will be given some antibiotics during the operation in the operating theatre to prevent infection
• Haematoma (collection of blood inside the breast) may occur if the drainage tubes cannot manage the amount of fluid. This is unusual and will normally occur while you are still hospitalized and may require a return visit to the operating theatre to evacuate the excess fluid. This if it happens does not influence the ultimate result
• Sensation in the nipple is preserved but may be temporarily reduced for up to 3 months postoperatively
• The scars run around the nipple margin as previously described or at the edge of the breast. My incisions are closed with buried stitches, which avoid unsightly stitch marks and produce the finest possible scar line. A few people do develop red unsightly scars – (hypertrophic scars) but fortunately this is rare, and can often be anticipated from a previous history of operation scars or accidents and there is a treatment, which helps control, this problem. Your scars will usually fade out progressively over a two year period
• Pre-existing asymmetry cannot always be fully corrected
• A seroma (collection of clear fluid) may require aspiration after the surgery but is usually self-limiting and doesn’t influence the ultimate result
After the operation
Your sutures will be removed on the 12th postoperative day. Sometimes the fine sutures around the areola will be removed earlier. The wound should be kept clean and dry until the removal of the sutures. It is possible to sit in a shallow bath and keep the dressings intact and dry.
You can drive 2 weeks after the operation if you did not have any wound healing problems. A full exercise program should be avoided for 6 weeks. You may be required to wear a compression garment for 6 weeks after the surgery.